Tom Myers mapped the continuous lines of fascia that run through your entire body. That map is why we can trace pain that has travelled far from where it started and identify the source with precision.
There is a question that almost every chronic pain patient has asked at some point. Why does treating the place that hurts so rarely produce lasting change? Why does the pain return, or shift to somewhere nearby, or turn out to be connected to something that seemed completely unrelated?
The answer lies in how the body is actually structured, as opposed to how we were taught to think about it. And the person who did more than anyone else to change that understanding is a manual therapist and anatomist called Tom Myers.
His work, Anatomy Trains, maps the body not as a collection of individual muscles with isolated functions but as a continuous network of connective tissue, Fascia, that links everything together into long, functional chains running from head to foot. He calls these chains myofascial meridians. At Physology, we have built our entire assessment system on this map because after more than two decades of clinical practice, it remains the most accurate explanation of chronic pain we have encountered and the one that consistently leads to the best outcomes for our patients.
What Are Anatomy Trains?
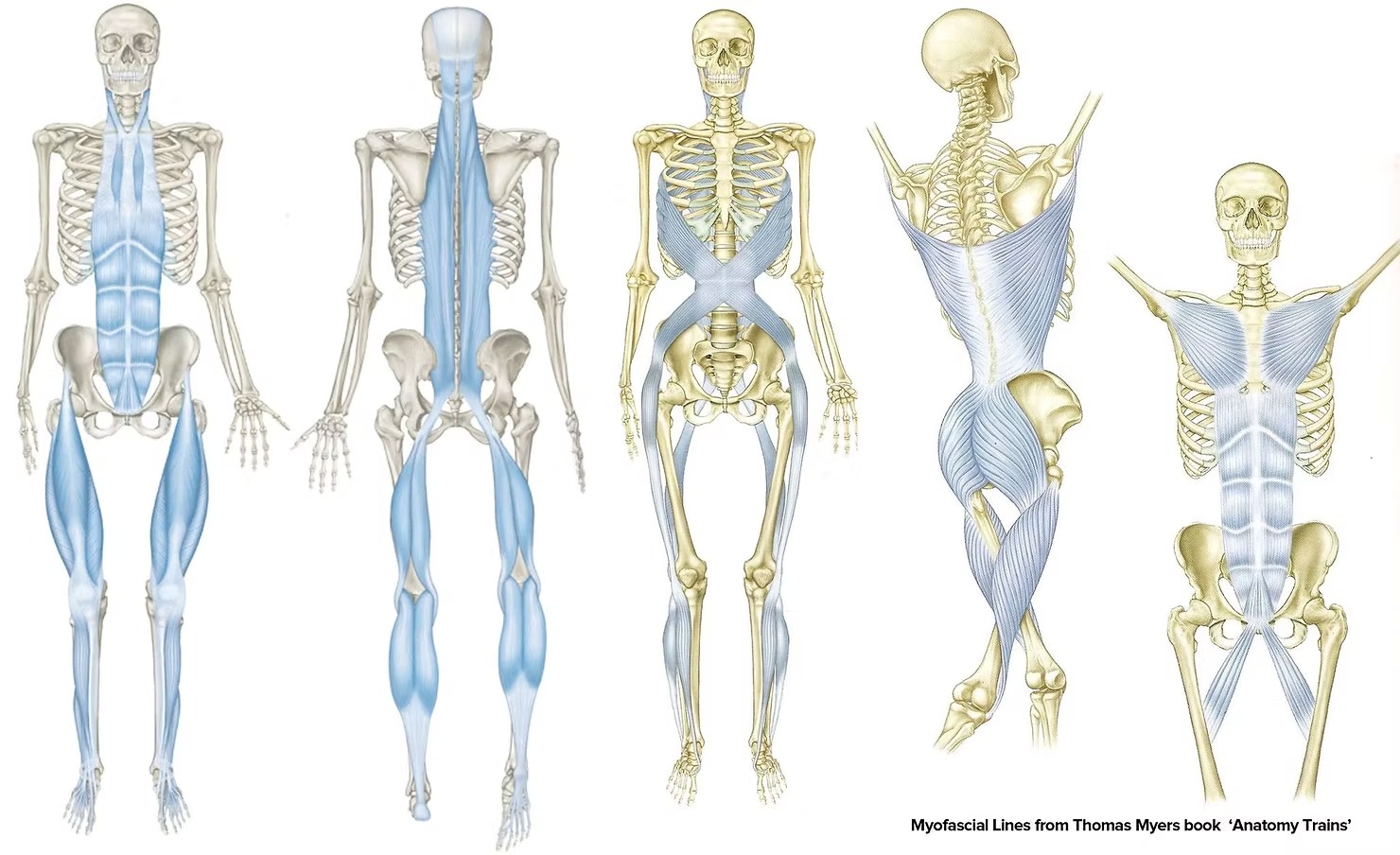
Tom Myers introduces the Anatomy Trains myofascial meridians
Think of your body like a tent: the poles are bones, the canvas is muscles, but the guy-lines and fabric holding everything together is Fascia. Tom Myers, a pioneer in Fascial anatomy, mapped how Fascia forms continuous lines that transmit force across the body. These are predictable pathways that explain why a tight calf can cause neck pain, or why poor posture pulls on your low back.
There are twelve main Anatomy Trains, each running the full length of the body and linking structures that conventional anatomy treats as unrelated. Pull on one part of a line and the tension travels. That is why chronic pain so often appears far from where it actually originates.
The Problem With the Old Maps
The muscle diagrams that have hung on the walls of GP surgeries and physiotherapy clinics for generations show muscles as independent units. Each one has an origin, an insertion, and an action. Treat the muscle, fix the problem. That is the model most practitioners are still working from.
That model is a starting point. What Fascia adds to it is the critical missing piece: in the living body, muscles are linked by Fascia into continuous lines of pull and tension that run throughout the whole body, and restriction in one part of that line creates effects at every other point along it.
The Anatomy Trains muscle maps. These replace the old red isolated muscle charts and show the true connected system.
Myers' map reflects what the body actually looks like when you approach it with an understanding of Fascia. It has been validated by dissection, replicated by researchers internationally, and applied clinically by practitioners working at the highest levels of elite sport for over two decades. Including at Physology.
Tom Myers explains Anatomy Trains at a talk for Google
The Myofascial Meridians
Myers identified twelve main lines of Fascial continuity running through the body. Each one transmits tension, distributes force, and when restricted, creates predictable patterns of pain and dysfunction. Here are the four most relevant to the chronic pain conditions we see most often at Physology.
Superficial Back Line
Runs from the plantar Fascia under your foot, up through the calf and hamstrings, up the spine, and over the skull to the forehead. A restriction anywhere along this line can create plantar fasciitis, tight hamstrings, chronic lower back pain, neck tension, and headaches, all connected through the same continuous Fascial chain.
Superficial Front Line
Runs from the top of the foot up through the shin, the front of the thigh, the abdomen, and the chest to the throat. Shortening here is a primary driver of forward head posture, breathing restriction, and the abdominal bracing that so often accompanies chronic back pain.
Spiral Line
Wraps around the body in a double helix, linking the skull to the opposite hip and continuing to the foot. When this line is imbalanced, it drives the rotation, twisting, and uneven loading patterns behind much of the chronic hip, knee, and low back pain that responds so well to a whole-line approach.
Deep Front Line
The deepest and most central line in the body, running from the inner arch of the foot up through the inner leg, through the psoas and the deep spinal muscles, and up to the base of the skull. This is the line most implicated in fibromyalgia, widespread chronic pain, and the chronic low back and pelvic pain that resists all conventional approaches.
The Tensegrity Model: Why the Whole Body Is Involved
To understand why Anatomy Trains matters so much, it helps to understand the structural principle that underpins it. The body works as a tensegrity structure, a term borrowed from architecture and engineering that combines tension and integrity.
Traditional anatomy described the skeleton as a compression structure, bones stacked on top of each other like a column of bricks, held in place by muscles. The body actually works more like a tent.
The poles float within a continuous network of tension created by the guy-ropes and canvas. Each pole is held in place by balanced tension from all directions. Pull on one guy-rope and the whole structure adjusts.
Your Fascial system is that network of tension. Your bones float within it. Your stability comes not from the bones stacking but from balanced tension distributed through the whole Fascial web. When part of that web is restricted, the whole body compensates. The skeleton shifts. Muscles overwork. Other areas of Fascia are placed under chronic strain. And pain appears, sometimes very far from the original restriction, because the whole structure has had to adapt.
This is why the same restriction can present differently in every patient, and why tracing pain back through the whole system consistently reveals a source that local treatment alone would never reach.
When you understand Anatomy Trains, a pattern emerges across conditions that seem unrelated. The Superficial Back Line connects plantar fasciitis to headaches. The Deep Front Line connects the inner arch of the foot to low back pain. The Spiral Line connects hip restriction to opposite shoulder problems. Here are some of the most common presentations we see, reframed through the Anatomy Trains lens.
Lower Back Pain
Almost always involves restriction in the Superficial Back Line and Deep Front Line, with drivers in the hamstrings, pelvis, and psoas rather than the lumbar spine itself.
Neck Pain
Often driven by restriction in the Superficial Front Line and Lateral Line from the chest and shoulders rather than the neck itself, which is simply the end of a much longer chain.
Headaches
The Superficial Back Line connects the plantar Fascia directly to the scalp and forehead. Chronic headaches frequently have their primary driver in the posterior chain, far below the head.
Fibromyalgia
Widespread Fascial restriction across multiple meridians, combined with the central sensitisation it creates, produces the diffuse, whole-body pain that characterises fibromyalgia and responds well to a whole-system Fascial approach.
Sciatica
Often not a disc problem at all. Piriformis restriction along the Spiral Line compresses the sciatic nerve in the buttock and creates identical symptoms to disc-related sciatica.
Plantar Fasciitis
A local diagnosis for a whole-line problem. The driver is almost always further up the Superficial Back Line, in the calf, hamstring, or even the lumbar spine.
How We Use Anatomy Trains
At Physology, the Anatomy Trains map is the foundation of our assessment process. Every patient we see is assessed as a whole system, not a collection of symptomatic sites. We follow the lines. We find the restrictions that are pulling the system out of balance. We treat the source, not the consequence.
Every patient we see brings a history of treatment at the site of pain. When we shift the assessment to the whole Fascial system, the restriction that is actually driving the symptoms becomes visible, often somewhere along the line that has never been examined before.
We combine the Anatomy Trains map with the dissection insights of Gill Hedley, whose integral anatomy series revealed the true connections within the Fascial body that only become visible when you approach the tissue with the intention of understanding it as a whole. Together, these frameworks give us a picture of the body that the conventional anatomical approach simply cannot provide.
The result is an assessment that most patients describe as the first time anyone has made sense of their symptoms. The connections between their various complaints, things they may have mentioned separately to different practitioners over the years, suddenly become visible as part of a single, coherent pattern. And once you can see the pattern, you can treat it properly.
Anatomy Trains is accepted science. Tom Myers' work has been validated by independent dissection studies, cited in peer-reviewed research internationally, and applied by medical teams working at the highest levels of professional sport for over twenty years.
We have been applying it in a Premier League context since 2013, beginning with Everton FC's first team medical staff and continuing today through direct work with professional players. The game has evolved and many elite players now manage their medical care independently outside club structures. We work directly with those players. The reason elite sport adopted this framework is consistent regardless of the structure: find the real cause, resolve it quickly, and prevent recurrence. The Anatomy Trains approach delivers that, which is why it has remained central to our work at that level.
What that credibility means in practice is that the thinking and assessment we bring to every patient in Bath and Bristol is the same quality that keeps professional athletes performing at the highest level. The understanding is the same. The commitment to finding the true source of pain is the same. Only the context is different.
Physology Bath & Bristol
Find Where Your Pain Really Starts
An Anatomy Trains assessment at Physology maps the whole system, traces restriction back to its source, and gives you a clear picture of what is actually driving your pain and what to do about it.
To understand the tissue that makes Anatomy Trains possible, read What Is Fascia? And to understand the specific process we use to take patients from chronic pain to pain-free, using this Anatomy Trains framework as its foundation, read about The Physology Method.
If you are dealing specifically with fibromyalgia or chronic back pain, our dedicated guides go much deeper into how the Anatomy Trains framework explains your condition and what treatment looks like: Fibromyalgia Focus Guide and Chronic Back Pain Guide.